
by John Halamka, Life as a Healthcare CIO
We began the meeting by relating our standards trajectory to today's agenda.
Our outstanding standards issues for discussion include
1. Content
Continued discussion of GreenCDA on the wire and overview of Stan Huff's CIMI initiative
Standardizing DICOM image objects for image sharing and investigating other possible approaches (e.g., cloud based JPEG2000 exchange). Consider image transfer standards, image viewing standards, and image reporting standards.
Query Health i.e. I2B2 distributed queries that send questions to data instead of requiring consolidation of data
Simplify the specification for quality measures to enhance consistency of implementation.
The December meeting included an overview of Query Health and Quality measure standards, leaving the discussion of GreenCDA/CIMI and DICOM to our 2012 meetings.
2. Vocabulary
Extend the quality measurement vocabularies to clinical summaries
Lab ordering compendium
The December meeting included a discussion of the lab ordering compendium, leaving the discussion of clinical summary vocabularies to our 2012 meetings.
3. Transport
Specify how the metadata ANPRM be integrated into the health exchange architecture
Additional NwHIN standards development (hearing re Exchange specification complexity, review/oversight of the S&I framework work on Exchange specifications simplification). Further define secure RESTful transport standards.
Accelerate provider directory pilots (Microdata, RESTful query/response that separates the transaction layer from the schema) and rapidly disseminate lessons learned.
The December meeting included an update on the provider directory and certificate components of transport
Our first presentation was an NCVHS update on ACA Section 10109 by Walter Suarez.
The Committee emphasized the need to coordinate NCHVS work and HITSC work given that division between administrative and clinical data is becoming less distinct over time
Our second presentation was an Implementation Workgroup Update by Liz Johnson about testing procedures that support the certification process.
The committee emphasized the need to pilot these procedures, ensuring they are as simple as possible and reflect a practical evaluation of the functionality intended to support policy goals.
Next, Doug Fridsma and Rich Elmore gave an ONC update. Rich Elmore described the Query Health initiative, as referenced in my previous blog post about sending questions to data (rather than sending data to registries).
The committee endorsed the work and noted that further research will be needed to link patients across multiple databases to avoid double counting individuals in quality measure denominators. The work of Jeff Jonas, as described in my earlier blog post about linking identity.
Doug updated the committee about the S&I Framework initiatives - Transitions of Care, Lab Results, Provider Directories, Data Segmentation (for privacy protection), and electronic submission of medical documentation for Medicare review.
We then discussed a preliminary framework for HITSC 2012 Workplan to ensure the items in the standards trajectory listed above are completed in 2012 as we continue to prepare for meaningful use stage 3.
A great meeting.
Wednesday, December 14, 2011
Monday, December 12, 2011
The Elephant in the Room
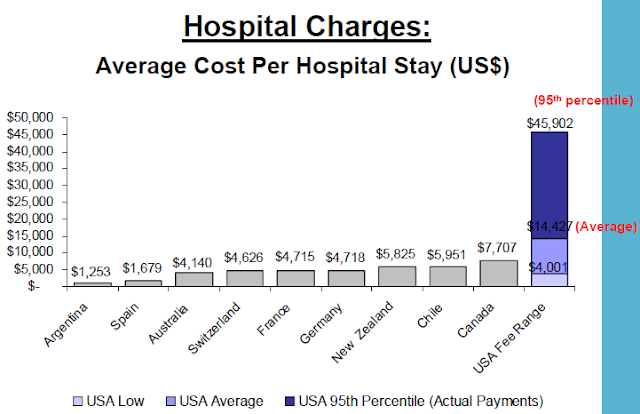
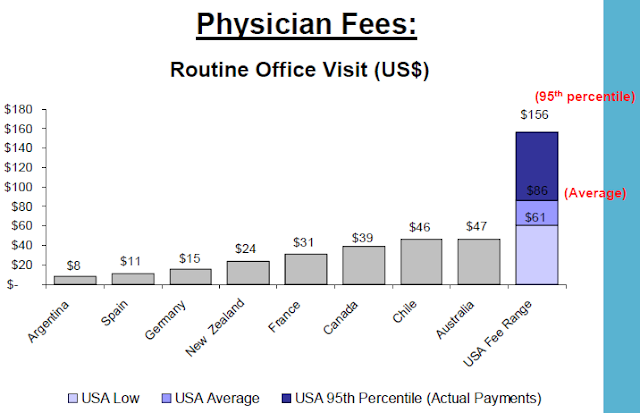
Why aren't we talking about pricing failures? The US, has consistently higher prices than any other country. The 2010 report by the International Federation of Health Plans consists of 23 pricing measures and the pattern is the same across each of these measures. And a 2010 investigation of Health Care Cost Trends and Cost Drivers in Massachusetts found that "price variations are correlated to market leverage..."
Before his departure from CMS, Don Berwick was interviewed by the New York Times and took a "parting shot at waste". Berwick listed five elements of waste including overtreatment of patients, failure to coordinate care, administrative complexity, burdensome rules and fraud. Pricing failures didn't make the list. (Many folks have commented and analyzed the five factors including John Halamka's terrific piece on how EHRs can address these 5 factors.)
Then in Berwick's December 7th speech to the IHI National Forum, he adds a sixth element:
Don Berwick defines pricing failures as "the waste that comes as prices migrate far from the actual costs of production plus fair profits." Think about that: "far from the actual costs of production plus fair profits". At a time when total healthcare expenditures consume a huge share of GDP and increasing at rates higher than inflation and wage increases, why haven't pricing failures been on the table? As we struggle to control costs and improve quality, there is intense focus on utilization, regulation and care coordination. Why not also focus on pricing failures?
So why hasn't pricing failures been part of the conversation up to now? Here's how the conversation usually proceeds: Health Affairs November 2011 article, Large Variations In Medicare Payments For Surgery Highlight Savings Potential From Bundled Payment Programs, "found that current Medicare episode payments for certain inpatient procedures varied by 49–130 percent across hospitals sorted into five payment groups. Intentional differences in payments attributable to such factors as geography or illness severity explained much of this variation. But after adjustment for these differences, per episode payments to the highest-cost hospitals were higher than those to the lowest-cost facilities by up to $2,549 for colectomy and $7,759 for back surgery."
Sounds like a clarion call for a focus on pricing failures doesn't it? Actually, no... The authors conclusions only speak to cost efficiency and utilization. "Our study suggests that bundled payments could yield sizable savings for payers, although the effect on individual institutions will vary because hospitals that were relatively expensive for one procedure were often relatively inexpensive for others. More broadly, our data suggest that many hospitals have considerable room to improve their cost efficiency for inpatient surgery and should look for patterns of excess utilization, particularly among surgical specialties, other inpatient specialist consultations, and various types of postdischarge care."
So is it time to broaden the conversation to include pricing failures? At least one health system has realized that "the jig is up". Perhaps it's time to peel the onion a bit... And take a serious look at pricing failures which deviate "far from the actual costs of production plus fair profits".
_______________________________
Background tables from the IFHP report:
Before his departure from CMS, Don Berwick was interviewed by the New York Times and took a "parting shot at waste". Berwick listed five elements of waste including overtreatment of patients, failure to coordinate care, administrative complexity, burdensome rules and fraud. Pricing failures didn't make the list. (Many folks have commented and analyzed the five factors including John Halamka's terrific piece on how EHRs can address these 5 factors.)
Then in Berwick's December 7th speech to the IHI National Forum, he adds a sixth element:
- "Overtreatment – the waste that comes from subjecting people to care that cannot possibly help them – care rooted in outmoded habits, supply-driven behaviors, and ignoring science.
- Failures of Coordination- the waste that comes when people – especially people with chronic illness – fall through the slats. They get lost, forgotten, confused. The result: complications, decays in functional status, hospital readmissions, and dependency.
- Failures of Reliability – the waste that comes with poor execution of what we know to do. The result: safety hazards and worse outcomes.
- Administrative Complexity – the waste that comes when we create our own rules that force people to do things that make no sense – that converts valuable nursing time into meaningless charting rituals or limited physician time into nonsensical and complex billing procedures.
- Pricing Failures – the waste that comes as prices migrate far from the actual costs of production plus fair profits.
- Fraud and Abuse – the waste that comes as thieves steal what is not theirs, and also from the blunt procedures of inspection and regulation that infect everyone because of the misbehaviors of a very few. We have estimated how big this waste is – from both the perspective of the Federal payers – Medicare and Medicaid – and for all payers."
Don Berwick defines pricing failures as "the waste that comes as prices migrate far from the actual costs of production plus fair profits." Think about that: "far from the actual costs of production plus fair profits". At a time when total healthcare expenditures consume a huge share of GDP and increasing at rates higher than inflation and wage increases, why haven't pricing failures been on the table? As we struggle to control costs and improve quality, there is intense focus on utilization, regulation and care coordination. Why not also focus on pricing failures?
So why hasn't pricing failures been part of the conversation up to now? Here's how the conversation usually proceeds: Health Affairs November 2011 article, Large Variations In Medicare Payments For Surgery Highlight Savings Potential From Bundled Payment Programs, "found that current Medicare episode payments for certain inpatient procedures varied by 49–130 percent across hospitals sorted into five payment groups. Intentional differences in payments attributable to such factors as geography or illness severity explained much of this variation. But after adjustment for these differences, per episode payments to the highest-cost hospitals were higher than those to the lowest-cost facilities by up to $2,549 for colectomy and $7,759 for back surgery."
Sounds like a clarion call for a focus on pricing failures doesn't it? Actually, no... The authors conclusions only speak to cost efficiency and utilization. "Our study suggests that bundled payments could yield sizable savings for payers, although the effect on individual institutions will vary because hospitals that were relatively expensive for one procedure were often relatively inexpensive for others. More broadly, our data suggest that many hospitals have considerable room to improve their cost efficiency for inpatient surgery and should look for patterns of excess utilization, particularly among surgical specialties, other inpatient specialist consultations, and various types of postdischarge care."
So is it time to broaden the conversation to include pricing failures? At least one health system has realized that "the jig is up". Perhaps it's time to peel the onion a bit... And take a serious look at pricing failures which deviate "far from the actual costs of production plus fair profits".
_______________________________
Background tables from the IFHP report:
Subscribe to:
Posts (Atom)






