
Healthcare Technology News has been selected by Medpedia to provide content to its newly launched News & Analysis site.
Medpedia, in association with Harvard Medical School, Stanford School of Medicine, UC Berkeley School of Public Health and University of Michigan Medical School, announced the launch of its News & Analysis site on November 10. "The Medpedia Project is a long-term, worldwide project to evolve a new model for sharing and advancing knowledge about health, medicine and the body among medical professionals and the general public. This model is founded on providing a free online technology platform that is collaborative, interdisciplinary and transparent."
Jennifer Hawkins at Medpedia described Medpedia's new strategy: "All of the bloggers on Medpedia News & Analysis as of today have been personally invited by us, the Medpedia team. We have searched the blogosphere for what we believe to be the best, most insightful blogs and everyone has been carefully chosen... All Blog feeds included in Medpedia's News & Analysis must be committed to sharing the highest quality medical and health information with the world."
Tuesday, November 24, 2009
Tuesday, November 17, 2009
H1N1: A Free-For-All in North America
 What has been the comparative response to the the H1N1 pandemic in Europe and the US? Belying claims that the Swine Flu response in the US is the precursor to a dysfunctional government run health system, the Europeans have this much more under control. An Associated Press review looked at this question. Highlights of that article follow:
What has been the comparative response to the the H1N1 pandemic in Europe and the US? Belying claims that the Swine Flu response in the US is the precursor to a dysfunctional government run health system, the Europeans have this much more under control. An Associated Press review looked at this question. Highlights of that article follow:"In Britain, there are no long lines of people seeking swine flue vaccine. Doctor's offices aren't swamped with desperate calls. And there are no cries of injustice that the vaccine is going to wealthy corporations or healthy people who don't really need it. Here, and across most of Europe, vaccine to protect against the pandemic flu is mostly given by invitation only to those at highest risk for flu complications.
Instead of advertising that vaccine had arrived and waiting for the lines to form, Britain's National Health Service sent letters, inviting all those who qualify to make an appointment and get the shots first.
Just this week, Americans learned that Wall Street giants Goldman Sachs and Citigroup got wine flu vaccine, even as many doctor's offices and community clinics still had none. The companies obtained the vaccine through standard procedures, and it was targeted to employees who met criteria for vaccination. But the perception of unfairness set off an outcry.
In the United Kingdom, the general population will be offered the shot after priority groups have been taken care of, probably in about two months.
Similar programs are being carried out in other European countries, all of which have socialized medicine:
- In Germany, doctors have also been contacting high-priority patients to come in for their swine flu shot, though other people who have asked for one have not been turned away.
- In Sweden, Denmark and Finland, some local governments are sending invitations to people in high-risk groups or posting information about vaccine availability on their Web sites.
- So far, France is only vaccinating health care workers. Its health minister said 6 million people in priority groups would start getting invitations to be vaccinated next week.
In North America, swine flu vaccination has largely been a free-for-all, although some U.S. states have recently beefed up their screening process to ensure pregnant women, children and people with health problems get shots before healthy older people."
Sunday, November 15, 2009
Biden: "We're going to cave in like crazy"
Vice President Joe Biden decides to fix health care while President Obama is out of the country. Saturday Night Live presents a message from the Vice President of the United States.
Tuesday, November 10, 2009
US Lags in Health IT for Primary Care
46% of U.S. primary care physicians report using electronic medical records (EMRs) significantly trailing other leading countries. EMRs are "nearly universal" in the Netherlands (99%), New Zealand (97%), the U.K. (96%), Australia (95%), Italy (94%), Norway (97%), and Sweden (94%).
The Commonwealth Fund report on A Survey of Primary Care Physicians in 11 Countries, 2009: Perspectives on Care Costs, and Experiences surveyed 10,000 primary care physicians in 11 countries. The findings: the United States lags far behind in terms of access to care, the use of financial incentives to improve the quality of care, and the use of health information technology.
The study's authors conclude that "the advanced health information technology and extensive use of quality incentives and care teams reported by Australian, Dutch, and New Zealand doctors reflect national payment and information system policies focused on primary care. Lacking such policies, the U.S. lags far behind its peers in these areas—even as it spends far more on health care overall. In addition, insurance coverage restrictions make it difficult for many U.S. physicians to provide their patients with timely access to care."
"We spend far more than any of the other countries in the survey, yet a majority of U.S. primary care doctors say their patients often can’t afford care, and a wide majority of primary care physicians don’t have advanced computer systems to access patient test results, anticipate and avoid medication errors, or support care for chronically ill patients," said Commonwealth Fund Senior Vice President Cathy Schoen, lead author of the article. "The patient-centered chronic care model originated in the U.S., yet other countries are moving forward faster to support care teams including nurses, spending time with patients, and assuring access to after-hours. The study underscores the pressing need for national reforms to close the performance gap to improve outcomes and reduce costs."
Seven of eleven countries surveyed had near universal deployment of EMRs and found EMRs with stronger functionality across all sizes of practices. By contrast in the US, more sophisticated EMR deployment was found primarily in larger practices and integrated care systems.
Clinical decision support is not that well developed across any of the countries surveyed. This included low scores for computerized reminders for treatment guidelines, tracking laboratory tests, and prompts to provide patients with test results.
The following are the comparative charts related to health information technology.






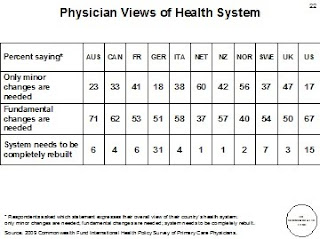
What are the salient differences in structure for primary care? "The United States is distinct in its reliance on internal medicine and pediatrics for primary care and its highly decentralized referral systems. The other countries rely extensively on general or family practice (GP/FP) physicians, often augmented by use of primary care nurses for preventive or chronic care and counseling. In Australia, Italy, the Netherlands, New Zealand, Norway, and the United Kingdom, patients register with primary care physicians, who typically serve as “gatekeepers” for referral for more specialized care. Other countries encourage registration through financial incentives for patients or providers, or both. Primary care practices, except in Sweden, generally operate as private practices. A majority of Swedish doctors work as public employees (local health centers), but reforms have been moving to private contracts and a mix of prepayment, or capitation, and fees. Australian, Canadian, French, German, and U.S. insurers generally pay fee-for-service (FFS). The other countries use a blend of capitation and fees for visits, targeted care, or performance incentives. The U.S. system includes examples of salary, mixed FFS and capitation, and integrated systems. Insurance systems differ across countries in patient cost sharing. In contrast to the United States, Canada, the Netherlands, and the United Kingdom have no or little cost sharing for medical care. France requires no cost sharing for specific chronic illnesses. Germany limits costs as a share of income. Norway and Sweden limit annual out-of-pocket costs. In Australia, primary care visits are often “bulkbilled” with no patient charge, and ceilings limit overall cost exposure. New Zealand has been reducing patient fees. Italy’s national benefits cover primary care in full, with copayments for outpatient drugs and specialists."
The study found that only the US had not pursued reform of primary care "including financial and information incentives... to provide a foundation for high-quality, efficient care."
The Commonwealth Fund report on A Survey of Primary Care Physicians in 11 Countries, 2009: Perspectives on Care Costs, and Experiences surveyed 10,000 primary care physicians in 11 countries. The findings: the United States lags far behind in terms of access to care, the use of financial incentives to improve the quality of care, and the use of health information technology.
The study's authors conclude that "the advanced health information technology and extensive use of quality incentives and care teams reported by Australian, Dutch, and New Zealand doctors reflect national payment and information system policies focused on primary care. Lacking such policies, the U.S. lags far behind its peers in these areas—even as it spends far more on health care overall. In addition, insurance coverage restrictions make it difficult for many U.S. physicians to provide their patients with timely access to care."
"We spend far more than any of the other countries in the survey, yet a majority of U.S. primary care doctors say their patients often can’t afford care, and a wide majority of primary care physicians don’t have advanced computer systems to access patient test results, anticipate and avoid medication errors, or support care for chronically ill patients," said Commonwealth Fund Senior Vice President Cathy Schoen, lead author of the article. "The patient-centered chronic care model originated in the U.S., yet other countries are moving forward faster to support care teams including nurses, spending time with patients, and assuring access to after-hours. The study underscores the pressing need for national reforms to close the performance gap to improve outcomes and reduce costs."
Seven of eleven countries surveyed had near universal deployment of EMRs and found EMRs with stronger functionality across all sizes of practices. By contrast in the US, more sophisticated EMR deployment was found primarily in larger practices and integrated care systems.
Clinical decision support is not that well developed across any of the countries surveyed. This included low scores for computerized reminders for treatment guidelines, tracking laboratory tests, and prompts to provide patients with test results.
The following are the comparative charts related to health information technology.







What are the salient differences in structure for primary care? "The United States is distinct in its reliance on internal medicine and pediatrics for primary care and its highly decentralized referral systems. The other countries rely extensively on general or family practice (GP/FP) physicians, often augmented by use of primary care nurses for preventive or chronic care and counseling. In Australia, Italy, the Netherlands, New Zealand, Norway, and the United Kingdom, patients register with primary care physicians, who typically serve as “gatekeepers” for referral for more specialized care. Other countries encourage registration through financial incentives for patients or providers, or both. Primary care practices, except in Sweden, generally operate as private practices. A majority of Swedish doctors work as public employees (local health centers), but reforms have been moving to private contracts and a mix of prepayment, or capitation, and fees. Australian, Canadian, French, German, and U.S. insurers generally pay fee-for-service (FFS). The other countries use a blend of capitation and fees for visits, targeted care, or performance incentives. The U.S. system includes examples of salary, mixed FFS and capitation, and integrated systems. Insurance systems differ across countries in patient cost sharing. In contrast to the United States, Canada, the Netherlands, and the United Kingdom have no or little cost sharing for medical care. France requires no cost sharing for specific chronic illnesses. Germany limits costs as a share of income. Norway and Sweden limit annual out-of-pocket costs. In Australia, primary care visits are often “bulkbilled” with no patient charge, and ceilings limit overall cost exposure. New Zealand has been reducing patient fees. Italy’s national benefits cover primary care in full, with copayments for outpatient drugs and specialists."
The study found that only the US had not pursued reform of primary care "including financial and information incentives... to provide a foundation for high-quality, efficient care."
Monday, November 2, 2009
House Bill May Finally Deliver on HIPAA's Promise
 HIPAA has never achieved its promise of standardized and ubiquitous electronic transactions. The House of Representatives will be voting this week on a Health Reform bill that
HIPAA has never achieved its promise of standardized and ubiquitous electronic transactions. The House of Representatives will be voting this week on a Health Reform bill that- requires electronic transaction standardization including elimination of payer-specific companion guides,
- enables the "real-time (or near real time) determination of an individual’s financial responsibility at the point of service and, to the extent possible, prior to service, including whether the individual is eligible for a specific service with a specific physician at a specific facility, on a specific date or range of dates, include utilization of a machine-readable health plan beneficiary identification card",
- enables near real-time adjudication of claims,
- requires "timely and transparent claim and denial management processes, including uniform claim edits, uniform reason and remark denial codes, tracking, adjudication, and appeal processing",
- requires a single binding companion guide starting with the X12 5010 electronic transaction set,
- requires implementation of the standards and new transactions within five years of enactment, and
- puts enforcement teeth behind use of the transactions.
SEC. 1173A. STANDARDIZE ELECTRONIC ADMINISTRATIVE TRANSACTIONS.
(a) STANDARDS FOR FINANCIAL AND ADMINISTRATIVE TRANSACTIONS.
(1) IN GENERAL.—The Secretary shall adopt and regularly update standards consistent with the goals described in paragraph (2).
(2) GOALS FOR FINANCIAL AND ADMINISTRATIVE TRANSACTIONS.—The goals for standards under paragraph (1) are that such standards shall, to the extent practicable—
(A) be unique with no conflicting or redundant standards;
(B) be authoritative, permitting no additions or constraints for electronic transactions, including companion guides;
(C) be comprehensive, efficient and robust, requiring minimal augmentation by paper transactions or clarification by further communications;
(D) enable the real-time (or near real time) determination of an individual’s financial responsibility at the point of service and, to the extent possible, prior to service, including whether the individual is eligible for a specific service with a specific physician at a specific facility, on a specific date or range of dates, include utilization of a machine-readable health plan beneficiary identification card or similar mechanism;
(E) enable, where feasible, near real-time adjudication of claims;
(F) provide for timely acknowledgment, response, and status reporting applicable to any electronic transaction deemed appropriate by the Secretary;
(G) describe all data elements (such as reason and remark codes) in unambiguous terms, not permit optional fields, require that data elements be either required or conditioned upon set values in other fields, and prohibit additional conditions except where required by (or
to implement) State or Federal law or to protect against fraud and abuse; and
(H) harmonize all common data elements across administrative and clinical transaction standards.
(3) TIME FOR ADOPTION.—Not later than 2 years after the date of the enactment of this section, the Secretary shall adopt standards under this section by interim, final rule.
(4) REQUIREMENTS FOR SPECIFIC STANDARDS.—The standards under this section shall be developed, adopted, and enforced so as to—
(A) clarify, refine, complete, and expand, as needed, the standards required under section
6 1173;
(B) require paper versions of standardized transactions to comply with the same standards as to data content such that a fully compliant, equivalent electronic transaction can be populated from the data from a paper version;
(C) enable electronic funds transfers, in order to allow automated reconciliation with the related health care payment and remittance advice;
(D) require timely and transparent claim and denial management processes, including uniform claim edits, uniform reason and remark denial codes, tracking, adjudication, and appeal processing;
(E) require the use of a standard electronic transaction with which health care providers may quickly and efficiently enroll with a health plan to conduct the other electronic transactions provided for in this part; and
(F) provide for other requirements relating to administrative simplification as identified by the Secretary, in consultation with stakeholders.
(5) BUILDING ON EXISTING STANDARDS.—In adopting the standards under this section, the Secretary shall consider existing and planned standards.
(6) IMPLEMENTATION AND ENFORCEMENT.— Not later than 6 months after the date of the enactment of this section, the Secretary shall submit to the appropriate committees of Congress a plan for the implementation and enforcement, by not later than 5 years after such date of enactment, of the standards under this section. Such plan shall include—
(A) a process and timeframe with milestones for developing the complete set of standards;
(B) a proposal for accommodating necessary changes between version changes and a process for upgrading standards as often as annually by interim, final rulemaking;
(C) programs to provide incentives for, and ease the burden of, implementation for certain health care providers, with special consideration given to such providers serving rural or underserved areas and ensure coordination with standards, implementation specifications, and certification criteria being adopted under the HITECH Act;
(D) programs to provide incentives for, and ease the burden of, health care providers who volunteer to participate in the process of setting standards for electronic transactions;
(E) an estimate of total funds needed to ensure timely completion of the implementation plan; and
(F) an enforcement process that includes timely investigation of complaints, random audits to ensure compliance, civil monetary and programmatic penalties for noncompliance consistent with existing laws and regulations, and a fair and reasonable appeals process building off of enforcement provisions under this part, and concurrent State enforcement jurisdiction. The Secretary may promulgate an annual audit and certification process to ensure that all health plans and clearinghouses are both syntactically and functionally compliant with all the standard transactions mandated pursuant to the administrative simplification provisions of this part and the Health Insurance Portability and Accountability Act of 1996.
(b) LIMITATIONS ON USE OF DATA.—Nothing in this section shall be construed to permit the use of information collected under this section in a manner that would violate State or Federal law.
(c) PROTECTION OF DATA.—The Secretary shall ensure (through the promulgation of regulations or otherwise) that all data collected pursuant to subsection (a) are used and disclosed in a manner that meets the HIPAA privacy and security law (as defined in section 3009(a)(2) of the Public Health Service Act), including any privacy or security standard adopted under section 3004 of such Act.
SEC. 1173B. INTERIM COMPANION GUIDES, INCLUDING OPERATING RULES.
(a) IN GENERAL.—The Secretary shall adopt a single, binding, comprehensive companion guide, that includes operating rules for each X12 Version 5010 transaction described in section 1173(a)(2), to be effective until the new version of these transactions which comply with
25 section 1173A are adopted and implemented.
(b) COMPANION GUIDE AND OPERATING RULES DEVELOPMENT.—In adopting such interim companion guide and rules, the Secretary shall comply with section 1172, except that a nonprofit entity that meets the following criteria shall also be consulted:
(1) The entity focuses its mission on administrative simplification.
(2) The entity uses a multistakeholder process that creates consensus-based companion guides, including operating rules using a voting process that ensures balanced representation by the critical stakeholders (including health plans and health care providers) so that no one group dominates the entity and shall include others such as standards development organizations, and relevant Federal or State agencies.
(3) The entity has in place a public set of guiding principles that ensure the companion guide and operating rules and process are open and transparent.
(4) The entity coordinates its activities with the HIT Policy Committee, and the HIT Standards Committee (established under title XXX of the Public Health Service Act) and complements the efforts of the Office of the National Healthcare Coordinator and its related health information exchange goals.
(5) The entity incorporates the standards issued under Health Insurance Portability and Accountability Act of 1996 and this part, and in developing the companion guide and operating rules does not change the definition, data condition or use of a data element or segment in a standard, add any elements or segments to the maximum defined data set, use any codes or data elements that are either marked ‘not used’ in the standard’s implementation specifications or are not in the standard’s implementation specifications, or change the meaning or intent of the standard’s implementation specifications.
(6) The entity uses existing market research and proven best practices.
(7) The entity has a set of measures that allow for the evaluation of their market impact and public reporting of aggregate stakeholder impact.
(8) The entity supports nondiscrimination and conflict of interest policies that demonstrate a commitment to open, fair, and nondiscriminatory practices.
(9) The entity allows for public reviews and comment on updates of the companion guide, including the operating rules.
(c) IMPLEMENTATION.—The Secretary shall adopt a single, binding companion guide, including operating rules under this section, for each transaction, to become effective with the X12 Version 5010 transaction implementation, or as soon thereafter as feasible. The companion guide, including operating rules for the transactions for eligibility for health plan and health claims status under this section shall be adopted not later than October 1, 2011, in a manner such that such set of rules is effective beginning not later than January 1, 2013. The companion guide, including operating rules for the remainder of the transactions described in section 1173(a)(2) shall be adopted not later than October 1, 2012, in a manner such that such set of rules is effective beginning not later than January 1, 2014.
(2) DEFINITIONS.—Section 1171 of such Act (42 U.S.C. 1320d) is amended— (A) in paragraph (1), by inserting ‘‘, and associated operational guidelines and instructions, as determined appropriate by the Secretary’’ after ‘‘medical procedure codes’’; and
(B) by adding at the end the following new paragraph:
(10) OPERATING RULES.—The term ‘operating rules’ means business rules for using and processing transactions, such as service level requirements, which do not impact the implementation specifications or other data content requirements.’’.
(3) CONFORMING AMENDMENT.—Section 1179(a) of such Act (42 U.S.C. 1320d–8(a)) is amended, in the matter before paragraph (1)—
(A) by inserting ‘‘on behalf of an indi1vidual’’ after ‘‘1978)’’; and
(B) by inserting ‘‘on behalf of an individual’’ after ‘‘for a financial institution’’ and
(b) STANDARDS FOR CLAIMS ATTACHMENTS AND COORDINATION OF BENEFITS.—
(1) STANDARD FOR HEALTH CLAIMS ATTACHMENTS.—Not later than 1 year after the date of the enactment of this Act, the Secretary of Health and Human Services shall promulgate an interim, final rule to establish a standard for health claims attachment transaction described in section 1173(a)(2)(B) of the Social Security Act (42 U.S.C. 1320d– 2(a)(2)(B)) and coordination of benefits.
(2) REVISION IN PROCESSING PAYMENT TRANSACTIONS BY FINANCIAL INSTITUTIONS.—
(A) IN GENERAL.—Section 1179 of the Social Security Act (42 U.S.C. 1320d–8) is amended, in the matter before paragraph (1)—
(i) by striking ‘‘or is engaged’’ and inserting ‘‘and is engaged’’; and
(ii) by inserting ‘‘(other than as a business associate for a covered entity)’’ after ‘‘for a financial institution’’.
(B) COMPLIANCE DATE.—The amendments made by subparagraph (A) shall apply to transactions occurring on or after such date (not later than January 1, 2014) as the Secretary of Health and Human Services shall specify.
(c) STANDARDS FOR FIRST REPORT OF INJURY.— Not later than January 1, 2014, the Secretary of Health and Human Services shall promulgate an interim final rule to establish a standard for the first report of injury transaction described in section 1173(a)(2)(G) of the Social Security Act (42 U.S.C. 1320d–2(a)(2)(G)).
(d) UNIQUE HEALTH PLAN IDENTIFIER.—Not later October 1, 2012, the Secretary of Health and Human Services shall promulgate an interim final rule to establish a unique health plan identifier described in section 1173(b) of the Social Security Act (42 U.S.C. 1320d– 2(b)) based on the input of the National Committee of Vital and Health Statistics and consultation with health plans, health care providers, and other interested parties.
(e) EXPANSION OF ELECTRONIC TRANSACTIONS IN MEDICARE.—Section 1862(a) of the Social Security Act (42 U.S.C. 1395y(a)) is amended—
(1) in paragraph (23), by striking ‘‘or’’ at the end;
(2) in paragraph (24), by striking the period and inserting ‘‘; or’’; and
(3) by inserting after paragraph (24) the following new paragraph: ‘‘(25) subject to subsection (h), not later than January 1, 2015, for which the payment is other than by electronic funds transfer (EFT) so long as the Secretary has adopted and implemented a standard for electronic funds transfer under section 1173A.’’.
(f) EXPANSION OF PENALTIES.—Section 1176 of such Act (42 U.S.C. 1320d–5) is amended by adding at the end the following new subsection:
(c) EXPANSION OF PENALTY AUTHORITY.—The Secretary may, in addition to the penalties provided under subsections (a) and (b), provide for the imposition of penalties for violations of this part that are comparable—
(1) in the case of health plans, to the sanctions the Secretary is authorized to impose under part C or D of title XVIII in the case of a plan that violates a provision of such part; or
(2) in the case of a health care provider, to the sanctions the Secretary is authorized to impose under part A, B, or D of title XVIII in the case of a health care provider that violations a provision of such part with respect to that provider.’’.
Monday, October 26, 2009
"Opt Out" Public Option is In
On Monday October 26, Senate Majority Leader Harry Reid called for the Senate health reform bill to include a public option. The bill will include a provision allowing states to opt out prior to 2014.
The Senate bill will be sent to the Congressional Budget Office for scoring within the next couple of days. Reid skirted the question as to whether he had the 60 votes needed to bring a vote to the Senate floor.
The much discussed trigger that would have delayed implementation of the public option will not be included nor scored. The bill will include the co-op provisions of the Senate Finance Committee bill.
C-Span reports that progressive Democratic senators refused to accept anything less than the public option, driving the final decision by the majority leader. Why the Opt Out? According to Reid, "we have 60 people in the caucus. It's comfort level - - we all hug together and see where we come out."
The Senate bill will be sent to the Congressional Budget Office for scoring within the next couple of days. Reid skirted the question as to whether he had the 60 votes needed to bring a vote to the Senate floor.
The much discussed trigger that would have delayed implementation of the public option will not be included nor scored. The bill will include the co-op provisions of the Senate Finance Committee bill.
C-Span reports that progressive Democratic senators refused to accept anything less than the public option, driving the final decision by the majority leader. Why the Opt Out? According to Reid, "we have 60 people in the caucus. It's comfort level - - we all hug together and see where we come out."
Guerilla Music at the AHIP Conference
On Friday October 23, America's Health Insurance Plans (AHIP) met in the aftermath of a tumultuous month in which the health insurance companies' lobbying operation released a study it commissioned which according to the White House is "an attempt to confuse the debate around health reform." The consequences of this ill-timed report could include building momentum for an end to the anti-trust exemptions that the insurance industry has enjoyed since 1945.
Just when the insurance industry must feel that it couldn't get any worse, attendees at the AHIP conference were subjected to this guerilla music by "Public Option Annie":
Just when the insurance industry must feel that it couldn't get any worse, attendees at the AHIP conference were subjected to this guerilla music by "Public Option Annie":
Thursday, October 15, 2009
October 14 HIT Standards Committee update
Guest author and Vice Chair of the HIT Standards Committee John Halamka reports on the October 14th meeting of the HIT Standards Committee, including important updates on patient access through portals, vocabulary standards, quality measures, security/privacy and the formation of a new implementation workgroup.
The October HIT Standards Committee meeting
by John Halamka
The day started with comments from David Blumenthal. He briefly described the Nationwide Healthcare Information Network (NHIN) as an evolving vital element of our national health information strategy. He emphasized that we need to expand the scope of our NHIN thinking to include consumer health information platforms in addition to the provider and government organizations that have been the focus to date. He also noted that we need to move from pilots/prototypes to scalable real world implementations, establishing the right governance mechanism for the NHIN.
The October HIT Standards Committee meeting
by John Halamka
The day started with comments from David Blumenthal. He briefly described the Nationwide Healthcare Information Network (NHIN) as an evolving vital element of our national health information strategy. He emphasized that we need to expand the scope of our NHIN thinking to include consumer health information platforms in addition to the provider and government organizations that have been the focus to date. He also noted that we need to move from pilots/prototypes to scalable real world implementations, establishing the right governance mechanism for the NHIN.
The Clinical Operations update followed and included a discussion of gaps in the current work. We started with a discussion of patient access to an EHR. Should we include clinical summaries, the entire record, or the standard data elements that can be exported to commercial PHRs such as Google Health and Microsoft Healthvault? We heard about experiences at Kaiser, Geisinger, BIDMC and others. It's clear that PHR data sharing is very heterogeneous at the moment and that convenience transactions such as appointment making, medication renewal, and referral management may be more important to patients than full access to every aspect of their record. The HIT Policy committee will be asked to define minimum requirements for patient access to EHR data.
We discussed needed enhancements to vocabularies including a national SNOMED-CT to ICD9/ICD10 mapping, RxNorm mapping to National Drug File Reference Terminology (NDF-RT) and Standard Product Labeling (SPL), a standard lab compendium for ordering, UCUM guidance and testing, and a national infrastructure to distribute and maintain codesets. I discussed this need for enhanced vocabulary tools in yesterday's blog. Our action item today was to create a Vocabulary sub-Workgroup that will address these issues and propose priorities and solutions to the entire Committee and ONC.
We heard an update from the Clinical Quality Workgroup about the re-tooling of quality measures to be more EHR-centric. Good progress is being made.
Next, we focused on privacy & security. Dixie Baker and Steve Findlay summarized a few updates to the standards matrix - SOAP 1.2 is the current recommended version and per evolving federal guidelines (NIST SP 800-63-1), Kerberos will be allowed but not required for 2011 because Federal systems will begin disallowing Kerberos in 2013. NIST SP 800-63-1 is cited as implementation guidance for "Level 2" certification criteria for authentication, but we've been careful not to impose Federal FISMA criteria on the private sector.
We discussed enhancements to privacy and security standards efforts, especially for 2013, including:
* A healthcare specific XML schema and vocabulary for representing subject, resource, action, and environmental attributes in security assertions i.e. SAML for healthcare
* A standard XML schema and vocabulary for representing consumer consents i.e. my CAML proposal
* Baseline security and privacy policies for the exchange of EHR information
* Standards for exchanges between the healthcare enterprise and the consumer
* Specification of Health Information Exchange assumptions and associated privacy and security policy. This relates to my blog yesterday in which I noted that policy guidance is really essential to pick the simplest set of security constructs needed to protect confidentiality.
Our action items today were
1. To spend the entire November HIT Standards Committee meeting hearing testimony from stakeholders on Security issues.
2. To work with ONC to ensure seamless communication and coordination between the HIT Policy Committee and HIT Standards Committee regarding privacy and security issues
3. To specify our assumptions for HIE information exchanges and share those assumptions with the Policy Committee so that they could specify a policy framework that then could serve as the basis for constraining security and privacy standards. One of our committee members noted that policy constrains architectural possibilities, enabling selection of the simplest set of standards needed to meet requirements.
Given the emphasis of the meeting on adoption and implementation, we discussed next steps regarding our new Implementation Workgroup. Specifically we will arrange for a day of testimony on October 29 from many stakeholder groups to better understand adoption and implementation issues, needs for enhanced implementation guidance, and identification of enablers that would accelerate interoperability such as new tools or filing standards gaps. We'll also conduct an online forum and accept written testimony. This feedback process is very important to ensure rapid cycle improvement in the standards making and standards selection processes. Per my blog yesterday, this will help with resolving the outstanding common data transport issues.
We ended the meeting with a discussion of the results from the privacy hearings conducted by the HIT Policy Committee on September 18.
Thus, we have action steps to resolve all the issues I raised on my blog yesterday - alignment of policy and standards activities to create the parsimonious set of security standards to protect confidentiality, a working group to resolve outstanding vocabulary issues, and a feedback process to resolve common data transport and other standards adoption/implementation issues.
A great meeting and I look forward to our day of implementation testimony on October 29 and our day of security testimony on November 19.
Tuesday, October 13, 2009
Blumenthal on Meaningful Use
Dr. David Blumenthal, National Coordinator for Health IT (ONC) has published an open letter on the Meaningful Use of Electronic Health Records. Blumenthal reported that CMS will issue it's proposed rule by year end.
___________________________________
 "Meaningful" Progress Toward Electronic Health Information Exchange
"Meaningful" Progress Toward Electronic Health Information Exchange
A Message from Dr. David Blumenthal, National Coordinator for Health Information Technology
I recently reported on our announcement of State Health Information Technology Grants and grants to establish Health Information Technology Regional Extension Centers, as authorized under the Health Information Technology for Economic and Clinical Health (HITECH) Act provisions of the American Recovery and Reinvestment Act of 2009 (the Recovery Act).
Today I want to discuss the important term “meaningful use” of electronic health records (EHRs) – both as a concept that underlies the movement toward an electronic health care environment and as a practical set of standards that will be issued as a proposed regulation by the end of 2009.
The HITECH Act provisions of the Recovery Act create a truly historic opportunity to transform our health system through unprecedented investments in the development of a nationwide electronic health information system. This system will ultimately help facilitate, inform, measure, and sustain improvements in the quality, efficiency, and safety of health care available to every American. Simply put, health professionals will be able to give better care, and their patients’ experience of care will improve, leading to better health outcomes overall.
As many of you are aware, the HITECH Act provides incentive payments to doctors and hospitals that adopt and meaningfully use health information technology. Eligible physicians, including those in solo or small practices, can receive up to $44,000 over five years under Medicare or $63,750 over six years under Medicaid for being meaningful users of certified electronic health records. Hospitals that become meaningful EHR users could receive up to four years of financial incentive payments under Medicare beginning in 2011, and up to six years of incentive payments under Medicaid beginning in October 2010.
The HITECH Act’s financial incentives demonstrate Congress’ and the Administration’s commitment to help those who want to improve their care delivery, and will serve as a catalyst to accelerate and smooth the path to HIT adoption by more individual providers and organizations. The dollars are tangible evidence of a national determination to bring health care into the 21st century.
The Office of the National Coordinator for Health Information Technology (ONC) is charged with coordinating nationwide efforts to implement and use the most advanced health information technology and the electronic exchange of health information. ONC is working with the Centers for Medicare & Medicaid Services (CMS), through an open and transparent process, on efforts to officially designate what constitutes “meaningful use.”
ONC has already engaged in a broad range of efforts to support the development of a formal definition of meaningful use. The HITECH Act designated a federal advisory committee, the HIT Policy Committee, with broad representation from major health care constituencies, to provide recommendations to ONC on meaningful use. The HIT Policy Committee has provided two sets of recommendations, informed by input from a variety of stakeholders. ONC and CMS have also conducted a series of listening sessions to solicit feedback from more than 200 representatives of various constituent groups and an open comment period where over 800 public comments were submitted and reviewed. The second set of recommendations on meaningful use was issued at a July 16 HIT Policy Committee meeting and details can be found at healthit.hhs.gov/policycommittee.
CMS is expected to publish a formal definition of meaningful use, for the purposes of receiving the Medicare and Medicaid incentive payments, by December 31, 2009. At that time, the public will be able to comment on the definition, and such comments will be considered in reaching any final definition of the term.
By focusing on “meaningful use,” we recognize that better health care does not come solely from the adoption of technology itself, but through the exchange and use of health information to best inform clinical decisions at the point of care. Meaningful use of EHRs, we anticipate, will also enable providers to reduce the amount of time spent on duplicative paperwork and gain more time to spend with their patients throughout the day. It will lead us toward improvements and sustainability of our health care system that can only be attained with the help of a reliable and secure nationwide electronic health information system.
The concept of meaningful use is simple and inspiring, but we recognize that it becomes significantly more complex at a policy and regulatory level. As a result, we expect that any formal definition of “meaningful use” must include specific activities health care providers need to undertake to qualify for incentives from the federal government.
Ultimately, we believe “meaningful use” should embody the goals of a transformed health system. Meaningful use, in the long-term, is when EHRs are used by health care providers to improve patient care, safety, and quality.
What’s next?
As stated above, the next step in our process is a notice of proposed rulemaking in late 2009 with a public comment period in early 2010. As this process unfolds, we will continue to talk and share experiences about transitioning to EHRs, and to help deepen understanding among physicians and hospitals about the use of EHRs. We will also present programs designed to help smooth the transition process, and identify activities physicians and hospitals can engage in now to promote adoption of EHRs. As efforts advance, we will turn our attention to other necessary supporting programs, some of which you will hear more about in the coming weeks, including defining what constitutes a “certified” EHR, which is one of the requirements to qualify for Medicare and Medicaid incentives.
In the meantime, what can providers do to move toward becoming “meaningful users” – even in the absence of a formal definition? Naturally, while understanding that the final definition will be adopted through a formal rulemaking process, it will be helpful to be as familiar as possible with the discussion of meaningful use criteria to date. (You will find that information posted at healthit.hhs.gov/meaningfuluse.)
Armed with an understanding of the discussion of meaningful use as it unfolds, providers can begin to consider how their own practices or organizations might be reshaped to enhance the efficiency and quality of care through the use of an electronic health record system. Be assured you will not be alone as you seek to adopt an EHR system. Through our recently announced collaborative HITECH grants programs and others to be initiated later this year, we will continue to support providers in moving forward. Additional details about the grants are also available in my previous update and at healthit.hhs.gov/HITECHgrants.
To some providers, particularly small or already stretched physician practices or small, rural hospitals, the path toward meaningful use may still seem arduous. To others, who would just prefer to stick with the “status quo,” it may seem like an unwanted intrusion. We believe that the time has come for coordinated action. The price of inaction – in adverse events, lost patient lives, delayed or improper treatments, unnecessary procedures, excessive costs, and so on – is just too high, and will only get worse.
There is much at stake and much to do. We must relieve the crushing burden of health care costs in this country by improving efficiency, and assuring the highest level of patient care and safety regardless of geography or demographics. By using current technologies in a meaningful way, as well as technology to be developed in the future, we will take great strides toward solving some of the most vexing problems facing our health care system and creating a new platform for innovative solutions to health care.
I look forward to providing periodic updates, and to continued interactions with all the communities that have so much to gain from this profound transformation.
Sincerely,
David Blumenthal, M.D., M.P.P.
National Coordinator for Health Information Technology
U.S. Department of Health & Human Services
___________________________________
 "Meaningful" Progress Toward Electronic Health Information Exchange
"Meaningful" Progress Toward Electronic Health Information ExchangeA Message from Dr. David Blumenthal, National Coordinator for Health Information Technology
I recently reported on our announcement of State Health Information Technology Grants and grants to establish Health Information Technology Regional Extension Centers, as authorized under the Health Information Technology for Economic and Clinical Health (HITECH) Act provisions of the American Recovery and Reinvestment Act of 2009 (the Recovery Act).
Today I want to discuss the important term “meaningful use” of electronic health records (EHRs) – both as a concept that underlies the movement toward an electronic health care environment and as a practical set of standards that will be issued as a proposed regulation by the end of 2009.
The HITECH Act provisions of the Recovery Act create a truly historic opportunity to transform our health system through unprecedented investments in the development of a nationwide electronic health information system. This system will ultimately help facilitate, inform, measure, and sustain improvements in the quality, efficiency, and safety of health care available to every American. Simply put, health professionals will be able to give better care, and their patients’ experience of care will improve, leading to better health outcomes overall.
As many of you are aware, the HITECH Act provides incentive payments to doctors and hospitals that adopt and meaningfully use health information technology. Eligible physicians, including those in solo or small practices, can receive up to $44,000 over five years under Medicare or $63,750 over six years under Medicaid for being meaningful users of certified electronic health records. Hospitals that become meaningful EHR users could receive up to four years of financial incentive payments under Medicare beginning in 2011, and up to six years of incentive payments under Medicaid beginning in October 2010.
The HITECH Act’s financial incentives demonstrate Congress’ and the Administration’s commitment to help those who want to improve their care delivery, and will serve as a catalyst to accelerate and smooth the path to HIT adoption by more individual providers and organizations. The dollars are tangible evidence of a national determination to bring health care into the 21st century.
The Office of the National Coordinator for Health Information Technology (ONC) is charged with coordinating nationwide efforts to implement and use the most advanced health information technology and the electronic exchange of health information. ONC is working with the Centers for Medicare & Medicaid Services (CMS), through an open and transparent process, on efforts to officially designate what constitutes “meaningful use.”
ONC has already engaged in a broad range of efforts to support the development of a formal definition of meaningful use. The HITECH Act designated a federal advisory committee, the HIT Policy Committee, with broad representation from major health care constituencies, to provide recommendations to ONC on meaningful use. The HIT Policy Committee has provided two sets of recommendations, informed by input from a variety of stakeholders. ONC and CMS have also conducted a series of listening sessions to solicit feedback from more than 200 representatives of various constituent groups and an open comment period where over 800 public comments were submitted and reviewed. The second set of recommendations on meaningful use was issued at a July 16 HIT Policy Committee meeting and details can be found at healthit.hhs.gov/policycommittee.
CMS is expected to publish a formal definition of meaningful use, for the purposes of receiving the Medicare and Medicaid incentive payments, by December 31, 2009. At that time, the public will be able to comment on the definition, and such comments will be considered in reaching any final definition of the term.
By focusing on “meaningful use,” we recognize that better health care does not come solely from the adoption of technology itself, but through the exchange and use of health information to best inform clinical decisions at the point of care. Meaningful use of EHRs, we anticipate, will also enable providers to reduce the amount of time spent on duplicative paperwork and gain more time to spend with their patients throughout the day. It will lead us toward improvements and sustainability of our health care system that can only be attained with the help of a reliable and secure nationwide electronic health information system.
The concept of meaningful use is simple and inspiring, but we recognize that it becomes significantly more complex at a policy and regulatory level. As a result, we expect that any formal definition of “meaningful use” must include specific activities health care providers need to undertake to qualify for incentives from the federal government.
Ultimately, we believe “meaningful use” should embody the goals of a transformed health system. Meaningful use, in the long-term, is when EHRs are used by health care providers to improve patient care, safety, and quality.
What’s next?
As stated above, the next step in our process is a notice of proposed rulemaking in late 2009 with a public comment period in early 2010. As this process unfolds, we will continue to talk and share experiences about transitioning to EHRs, and to help deepen understanding among physicians and hospitals about the use of EHRs. We will also present programs designed to help smooth the transition process, and identify activities physicians and hospitals can engage in now to promote adoption of EHRs. As efforts advance, we will turn our attention to other necessary supporting programs, some of which you will hear more about in the coming weeks, including defining what constitutes a “certified” EHR, which is one of the requirements to qualify for Medicare and Medicaid incentives.
In the meantime, what can providers do to move toward becoming “meaningful users” – even in the absence of a formal definition? Naturally, while understanding that the final definition will be adopted through a formal rulemaking process, it will be helpful to be as familiar as possible with the discussion of meaningful use criteria to date. (You will find that information posted at healthit.hhs.gov/meaningfuluse.)
Armed with an understanding of the discussion of meaningful use as it unfolds, providers can begin to consider how their own practices or organizations might be reshaped to enhance the efficiency and quality of care through the use of an electronic health record system. Be assured you will not be alone as you seek to adopt an EHR system. Through our recently announced collaborative HITECH grants programs and others to be initiated later this year, we will continue to support providers in moving forward. Additional details about the grants are also available in my previous update and at healthit.hhs.gov/HITECHgrants.
To some providers, particularly small or already stretched physician practices or small, rural hospitals, the path toward meaningful use may still seem arduous. To others, who would just prefer to stick with the “status quo,” it may seem like an unwanted intrusion. We believe that the time has come for coordinated action. The price of inaction – in adverse events, lost patient lives, delayed or improper treatments, unnecessary procedures, excessive costs, and so on – is just too high, and will only get worse.
There is much at stake and much to do. We must relieve the crushing burden of health care costs in this country by improving efficiency, and assuring the highest level of patient care and safety regardless of geography or demographics. By using current technologies in a meaningful way, as well as technology to be developed in the future, we will take great strides toward solving some of the most vexing problems facing our health care system and creating a new platform for innovative solutions to health care.
I look forward to providing periodic updates, and to continued interactions with all the communities that have so much to gain from this profound transformation.
Sincerely,
David Blumenthal, M.D., M.P.P.
National Coordinator for Health Information Technology
U.S. Department of Health & Human Services
Thursday, October 8, 2009
CBO Scores - Does Health Reform Win?
The Congressional Budget Office has released their analysis of the costs and revenues attached to the Senate Finance Committee's Health Reform bill.
 By the numbers:
By the numbers:
29 million Additional insured (by 2019)
25 million Uninsured (by 2019)
94% Total non-elderly legal residents with health insurance
(up from 83%)
91% Total non-elderly residents with health insurance
13% Maximum % of income to be spent on health insurance
$345 billion Expansion of Medicaid and Children's Health Insurance
$461 billion Subsidies for Insurance
$ 23 billion Small Employer Tax credits
========
$829 billion Gross 10 year cost of coverage provisions
($ 4) billion Penalty payments for uninsured individuals
($ 23) billion Penalty payments for employers
($201) billion Excise tax on high premium insurance plans
($ 83) billion Other effects on tax revenues and outlays
=========
$518 billion Net 10 year cost of coverage provisions
$599 billion Offsetting Medicare savings and increased tax revenues
($ 81) billion 10 year reduction in federal deficit
Senate Finance Committee will vote on the bill after Senator Olympia Snowe has had time to review the CBO analysis, likely by next week.
By the numbers:29 million Additional insured (by 2019)
25 million Uninsured (by 2019)
94% Total non-elderly legal residents with health insurance
(up from 83%)
91% Total non-elderly residents with health insurance
13% Maximum % of income to be spent on health insurance
$345 billion Expansion of Medicaid and Children's Health Insurance
$461 billion Subsidies for Insurance
$ 23 billion Small Employer Tax credits
========
$829 billion Gross 10 year cost of coverage provisions
($ 4) billion Penalty payments for uninsured individuals
($ 23) billion Penalty payments for employers
($201) billion Excise tax on high premium insurance plans
($ 83) billion Other effects on tax revenues and outlays
=========
$518 billion Net 10 year cost of coverage provisions
$599 billion Offsetting Medicare savings and increased tax revenues
($ 81) billion 10 year reduction in federal deficit
Senate Finance Committee will vote on the bill after Senator Olympia Snowe has had time to review the CBO analysis, likely by next week.
Preliminary Analysis of the Senate Finance Committee Chairman’s Mark As Amended
CBO and the staff of the Joint Committee on Taxation (JCT) have just issued a preliminary analysis of the Senate Finance Committee Chairman’s mark for the America’s Healthy Future Act of 2009, incorporating the amendments that have been adopted to date by the committee. That analysis reflects the specifications posted on the committee’s Web site on October 2, 2009, corrections posted on October 5, and additional clarifications provided by the staff of the committee through October 6. CBO and JCT’s analysis is preliminary in large part because the Chairman’s mark, as amended, has not yet been embodied in legislative language.
Among other things, the Chairman’s mark, as amended, would establish a mandate for most legal residents of the United States to obtain health insurance; set up insurance “exchanges” through which certain individuals and families could receive federal subsidies to substantially reduce the cost of purchasing that coverage; significantly expand eligibility for Medicaid; substantially reduce the growth of Medicare’s payment rates for most services (relative to the growth rates projected under current law); impose an excise tax on insurance plans with relatively high premiums; and make various other changes to the Medicaid and Medicare programs and the federal tax code.
According to CBO and JCT’s assessment, enacting the Chairman’s mark, as amended, would result in a net reduction in federal budget deficits of $81 billion over the 2010–2019 period. The estimate includes a projected net cost of $518 billion over 10 years for the proposed expansions in insurance coverage. That net cost itself reflects a gross total of $829 billion in credits and subsidies provided through the exchanges, increased net outlays for Medicaid and the Children’s Health Insurance Program (CHIP), and tax credits for small employers; those costs are partly offset by $201 billion in revenues from the excise tax on high-premium insurance plans and $110 billion in net savings from other sources. The net cost of the coverage expansions would be more than offset by the combination of other spending changes that CBO estimates would save $404 billion over the 10 years and other provisions that JCT and CBO estimate would increase federal revenues by $196 billion over the same period. In subsequent years, the collective effect of those provisions would probably be continued reductions in federal budget deficits. Those estimates are all subject to substantial uncertainty.
By 2019, CBO and JCT estimate, the number of nonelderly people who are uninsured would be reduced by about 29 million, leaving about 25 million nonelderly residents uninsured (about one-third of whom would be unauthorized immigrants). Under the proposal, the share of legal nonelderly residents with insurance coverage would rise from about 83 percent currently to about 94 percent. Roughly 23 million people would purchase their own coverage through the new insurance exchanges, and there would be roughly 14 million more enrollees in Medicaid and CHIP than is projected under current law. Relative to currently projected levels, the number of people either purchasing individual coverage outside the exchanges or obtaining coverage through employers would decline by several million.
Although CBO does not generally provide cost estimates beyond the 10 year budget projection period (2010 through 2019 currently), Senate rules require some information about the budgetary impact of legislation in subsequent decades, and many Members have requested CBO analyses of the long-term budgetary impact of broad changes in the nation’s health care and health insurance systems. However, a detailed year-by-year projection, like those that CBO prepares for the 10-year budget window, would not be meaningful because the uncertainties involved are simply too great. CBO has therefore developed a rough outlook for the decade following the 10-year budget window by grouping the elements of the proposal into broad categories and assessing the rate at which the budgetary impact of each of those broad categories is likely to increase over time.
All told, the proposal would reduce the federal deficit by $12 billion in 2019, CBO and JCT estimate. After that, the added revenues and cost savings are projected to grow more rapidly than the cost of the coverage expansion. Consequently, CBO expects that the proposal, if enacted, would reduce federal budget deficits over the ensuing decade relative to those projected under current law—with a total effect during that decade that is in a broad range between one-quarter percent and one-half percent of GDP. The imprecision of that calculation reflects the even greater degree of uncertainty that attends to it, compared with CBO’s 10-year budget estimates.
These projections assume that the proposals are enacted and remain unchanged throughout the next two decades, which is often not the case for major legislation. For example, the sustainable growth rate (SGR) mechanism governing Medicare’s payments to physicians has frequently been modified (either through legislation or administrative action) to avoid reductions in those payments. The projected savings for the proposal reflect the cumulative impact of a number of specifications that would constrain payment rates for providers of Medicare services. The long-term budgetary impact could be quite different if those provisions were ultimately changed or not fully implemented. (If those changes arose from future legislation, CBO would estimate their costs w
Tuesday, October 6, 2009
Patient-Centered Medical Home Demo Improves Quality and Patient Sat
A demonstration project by Group Health found that the Patient-Centered Medical Home (PCMH) "redesign can be associated with improvements in patient experience, clinician burnout, and quality without increasing overall cost."
With PCMH, Group Health found that the patients' experience was rated higher on 6 out of 7 indicators without an increase in costs. "For staff burnout, 10% of PCMH staff reported high emotional exhaustion at 12 months compared with 30% of controls, despite similar rates at baseline. PCMH patients also had gains in composite quality between 1.2% and 1.6% greater than those of other patients. PCMH patients used more e-mail, phone, and specialist visits, but fewer emergency services. At 12 months, there were no significant differences in overall costs."
 Prior to the PCMH demonstration project, Group Health had implemented access and efficiency improvements which increased patient satisfaction but also increase physician fatigue. The improvements had included "same-day appointment scheduling, direct access to some specialists, primary care redesign to enhance care efficiency, variable physician compensation (salaries with relative value unit [RVU] incentives), and an electronic medical record with a patient Web portal to enable patient e-mail, online medication refills, and record review. The reforms succeeded in improving patient access and satisfaction, but also increased physician workload, as evidenced by larger panel sizes, greater resource intensity per face-to-face visit, and increasing adoption of patient e-mail. These workload changes, combined with the implementation of the electronic medical record, resulted in fatigue and decreased work satisfaction. Relative reductions also were seen in nationally reported quality-of-care indicators as well as downstream utilization increases in specialty care, emergency care, and inpatient days."
Prior to the PCMH demonstration project, Group Health had implemented access and efficiency improvements which increased patient satisfaction but also increase physician fatigue. The improvements had included "same-day appointment scheduling, direct access to some specialists, primary care redesign to enhance care efficiency, variable physician compensation (salaries with relative value unit [RVU] incentives), and an electronic medical record with a patient Web portal to enable patient e-mail, online medication refills, and record review. The reforms succeeded in improving patient access and satisfaction, but also increased physician workload, as evidenced by larger panel sizes, greater resource intensity per face-to-face visit, and increasing adoption of patient e-mail. These workload changes, combined with the implementation of the electronic medical record, resulted in fatigue and decreased work satisfaction. Relative reductions also were seen in nationally reported quality-of-care indicators as well as downstream utilization increases in specialty care, emergency care, and inpatient days."
The implementation of the Patient-Centered Medical Home was organized around the relationship between the primary care physician and the patient. The primary care physician leads the clinical team and coordinates the planning of care with the patient. "Maximum use of technology" facilitates patient access.
Group Health implemented changes related to the structure of the care teams, point-of-care, patient outreach and management. Changes included "the use of team huddles, previsit outreach and chart review, and use of patient-centered quality deficiency reports. The PCMH clinic emphasized both e-mail and telephone encounters (as an alternative or complement to in-person visits), depending on patient abilities and preferences."

As a result of its success, Group Health is expanding its Patient-Centered Medical Home program to all of its centers.
With PCMH, Group Health found that the patients' experience was rated higher on 6 out of 7 indicators without an increase in costs. "For staff burnout, 10% of PCMH staff reported high emotional exhaustion at 12 months compared with 30% of controls, despite similar rates at baseline. PCMH patients also had gains in composite quality between 1.2% and 1.6% greater than those of other patients. PCMH patients used more e-mail, phone, and specialist visits, but fewer emergency services. At 12 months, there were no significant differences in overall costs."
 Prior to the PCMH demonstration project, Group Health had implemented access and efficiency improvements which increased patient satisfaction but also increase physician fatigue. The improvements had included "same-day appointment scheduling, direct access to some specialists, primary care redesign to enhance care efficiency, variable physician compensation (salaries with relative value unit [RVU] incentives), and an electronic medical record with a patient Web portal to enable patient e-mail, online medication refills, and record review. The reforms succeeded in improving patient access and satisfaction, but also increased physician workload, as evidenced by larger panel sizes, greater resource intensity per face-to-face visit, and increasing adoption of patient e-mail. These workload changes, combined with the implementation of the electronic medical record, resulted in fatigue and decreased work satisfaction. Relative reductions also were seen in nationally reported quality-of-care indicators as well as downstream utilization increases in specialty care, emergency care, and inpatient days."
Prior to the PCMH demonstration project, Group Health had implemented access and efficiency improvements which increased patient satisfaction but also increase physician fatigue. The improvements had included "same-day appointment scheduling, direct access to some specialists, primary care redesign to enhance care efficiency, variable physician compensation (salaries with relative value unit [RVU] incentives), and an electronic medical record with a patient Web portal to enable patient e-mail, online medication refills, and record review. The reforms succeeded in improving patient access and satisfaction, but also increased physician workload, as evidenced by larger panel sizes, greater resource intensity per face-to-face visit, and increasing adoption of patient e-mail. These workload changes, combined with the implementation of the electronic medical record, resulted in fatigue and decreased work satisfaction. Relative reductions also were seen in nationally reported quality-of-care indicators as well as downstream utilization increases in specialty care, emergency care, and inpatient days."The implementation of the Patient-Centered Medical Home was organized around the relationship between the primary care physician and the patient. The primary care physician leads the clinical team and coordinates the planning of care with the patient. "Maximum use of technology" facilitates patient access.
Group Health implemented changes related to the structure of the care teams, point-of-care, patient outreach and management. Changes included "the use of team huddles, previsit outreach and chart review, and use of patient-centered quality deficiency reports. The PCMH clinic emphasized both e-mail and telephone encounters (as an alternative or complement to in-person visits), depending on patient abilities and preferences."

As a result of its success, Group Health is expanding its Patient-Centered Medical Home program to all of its centers.
Monday, September 28, 2009
Discharge Summaries Grossly Inadequate at Documenting Pending Test Results
A study in the September edition of the Journal of General Internal Medicine found that "discharge summaries are grossly inadequate at documenting both tests with pending results and the appropriate follow-up providers."
The study found that only 13% of discharge summaries document all pending tests. And only 25% of discharge summaries mention some pending tests. Follow-up providers information was included in 67% of discharge summaries. "The documentation rate for pending tests was not associated with level of experience of the provider preparing the summary, patient’s age or race, length of hospitalization, or duration it took for results to return." The study evaluated discharge summaries at two academic medical centers for patients that had pending test results.
 This adds to the communication challenges referring physicians face coordinating care in follow-up to a hospital visit. Yet communications issues are accountable for over half of all preventable errors. And communications issues are twice as likely to be related to deaths as compared to "clinical inadequacy".
This adds to the communication challenges referring physicians face coordinating care in follow-up to a hospital visit. Yet communications issues are accountable for over half of all preventable errors. And communications issues are twice as likely to be related to deaths as compared to "clinical inadequacy".
The study reported that approximately 41% of patient are discharged with pending test results and 9% of these test results affect patient care management.
The study found that only 13% of discharge summaries document all pending tests. And only 25% of discharge summaries mention some pending tests. Follow-up providers information was included in 67% of discharge summaries. "The documentation rate for pending tests was not associated with level of experience of the provider preparing the summary, patient’s age or race, length of hospitalization, or duration it took for results to return." The study evaluated discharge summaries at two academic medical centers for patients that had pending test results.
This adds to the communication challenges referring physicians face coordinating care in follow-up to a hospital visit. Yet communications issues are accountable for over half of all preventable errors. And communications issues are twice as likely to be related to deaths as compared to "clinical inadequacy".The study reported that approximately 41% of patient are discharged with pending test results and 9% of these test results affect patient care management.
Subscribe to:
Posts (Atom)






