The
Center for Information Technology Leadership (CITL) has estimated that Personal Health Records (PHR) can deliver
savings of $21 billion annually.
Architectures
CITL's full report
evaluated four different PHR architectures: 1) Provider-tethered, 2) Payer-tethered, 3) Third party and 4) Interoperable.
Tethered architectures refer to providers or payers providing the data integration to the PHR. The
Third Party architecture refers to manual aggregation of health information but without the ability to integrate back to the clinical and administrative systems "in their native formats". In the
Interoperable architecture, patient information flows into the PHR using standards based health information exchange from sources throughout the region and from there can be machine interpreted by the clinical and administrative systems.

CostsThe Provider-tethered architecture provides a limited view of the patient, compared to an interoperable regional approach. This architecture also requires a very large number of implementations to support 80% PHR adoption:
- Provider - 26,000
- Payer - 706
- Third Party - 3
- Interoperable - 428
The number of implementations is a major factor driving the total national installation costs.


SavingsThe CITL value chain model is used to estimate the value of the PHR functions including:
1. Information Sharing1a. Complete Test results
1b. Complete Medication lists
2. Information Self-management2a. Congestive Heart Failure Management
2b. Smoking Cessation Management
3. Information Exchange 3a. Appointment Scheduling
3b. Medication Renewals
3c. Pre-Encounter Questionnaire
3d. e-Visits

Four of these functions contribute 95% of the value: Sharing of complete test results ($7.9); Congestive heart failure management ($6.3), e-Visits ($4.8), and Medication renewals ($1.1).
The annual steady state net value for the Interoperable architecture comes in tops at $19 billion, followed by Third-Party and Payer-tethered at $11 billion with
Provider-tethered trailing at a whopping negative $29 billion.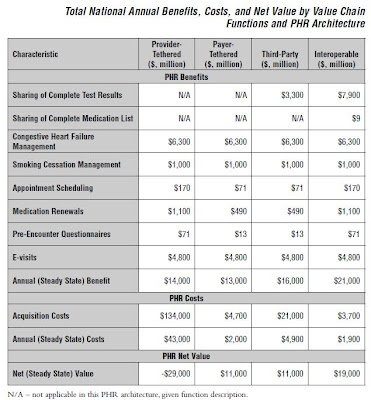
News Analysis
So what are the strategic implications for Healthcare Organizations (HCO's)?
- HCO's won't be able to carry this on their shoulders - - the costs are prohibitive.
- HCO's will need to ensure that their clinical and administrative systems can interoperate using national standards and can participate in regional health information exchange initiatives.
- HCO's should look to collaborate and invest in PHR's that are building towards an interoperable standards-based technology platform and are able to connect with multiple providers in the region.
- HCO's will need to develop strategies which distinguish between the 1) Personal Health Record (patient-centered) and 2) the portals which connect the HCO to the patient/consumer (HCO-centered).
The strategic implications align well with a recent presentation to AHIC of
PHR adoption which favored a Utility Service Model.
Many thanks to Blackford Middleton and CITL for permission to reproduce excerpts from the report.














