The study was conducted in 41 Texas hospitals representing a cross-section of hospital types and sizes with data on 167,233 patients over the age of 50.
The key finding: “Hospitals with automated notes and records, order entry, and clinical decision support had fewer complications, lower mortality rates, and lower costs.” The study does not conclude that there is any causal relationship from technology to outcomes and cost, but does describe the very strong correlation between them.

One of the study's authors, Dr. Ruben Amarasingham, Associate Chief of Medicine for Parkland Health and Hospital System, graciously agreed to sit down with Healthcare Technology News (HTN) to describe these results.
HTN: Congratulations on your study - - very compelling results, on such a large scale.
Amarasingham: Thank you very much. We think its one of the largest studies to evaluate the relationship between technology, clinical effectiveness and cost. We looked at this using a new framework for measuring health information technology, the Clinical Information Technology Assessment Tool (CITAT).
HTN: Can you explain CITAT? Please break it down for us.
Amarasingham: We started to develop the tool 5 years ago, starting in 2003. When we looked at HIS systems, we found that there was no good method to evaluate hospitals against each other. If hospitals say they've implemented an EMR, it's impossible to know if the definitions, functionality, usability and maturation are the same across hospitals. We therefore started with a universe of activities that physicians do in a hospital - - thousands of activities. If the activity is electronic, regardless of the specific software/technology, we asked physicians how would they respond to the following:
1) Do you have electronic support for this activity?
2) Do you know how to use the technology for this activity?
3) Do you choose to use the technology for this activity?
From that we created an instrument based on what we, and others, thought were the most important clinical activities and scaled a hospital based on whether its physicians are using the technology. We set a very high bar – the hospital needed to have the technology and the physician not only needed to know how to use the technology, but then had to choose to use it over other processes (like falling back to paper or having an assistant deal with the technology). It’s entirely possible for a hospital to spend millions and still fail on these criteria.
HTN: What piqued your interest in this?
Amarasingham: I'm an inpatient physician myself so it is a natural set of questions to ask. As a Robert Woods Johnson Clinical Scholar at Johns Hopkins, my mentors pushed me to define how to quantitatively measure information technology and the effect on clinical outcomes. Many of the technology studies were worrisome - it was not clear that the technology measure could be generalized. There was less attention to real usability. After studying the human factors research, particularly
Vimla Patel's work at Columbia, it became clear that these three criteria of physician use were very important. We published an
earlier study that described and validated the CITAT tool.
HTN: The data is so compelling regarding the reductions in mortality and complications. Do you have any sense for the key drivers?
Amarasingham: We suggest some possibilities in our paper. Smaller earlier studies found similar reductions and specifically examined in qualitative ways how technology might mediate these outcomes. I think that hospital medicine is extraordinarily complex with ever more studies and more innovations. Every day physicians are presented with multiple choices of treatment and diagnostics. Which parameters should be monitored? How do we track an illness over time? Information systems help manage all the information that is available in terms of decision support.
On top of the knowledge explosion, care is increasingly fragmented. There are multiple teams of physicians and para-physicians, shift work, etc. - - a growing and large number of actors just within the theater of medicine. A good IT system may help coordinate care; becoming perhaps a member of the team by helping to facilitate communication among staff who are working different shifts and schedules. In my opinion, the coordination of care makes an enormous difference in an increasingly fragmented medical system.
Good information systems also possess a certain degree of artificial intelligence. Physicians may not track the small trends in the patient’s condition. Presenting alerts and information in an objective way that may help physicians know where to look is so important. Conversely, poorly constructed systems have the potential to be harmful.
HTN: Why wasn’t Length of Stay related to use of technology?
Amarasingham: Length of Stay (LOS) is probably at the lowest it could be in American hospitals. A
2005 National Discharge Survey examined LOS over 30 years. It has been systematically driven down by a number of pressures, including attention by payers and regulators. Given the very small lengths of stay, it's possible that information technology provides efficiencies but not enough to change an already low LOS.
HTN: You published a report earlier this year which found that
academic affiliation and larger IT operating, capital, and staff budgets are associated with more highly automated clinical information systems. Basic conclusion: more investment, more highly automated systems – simple. So why in this study do you find that higher levels of automation of test results, order entry and decision support are all contributing to lower costs? It seems almost contradictory.
Amarasingham: Great question. We found the hospitals that had better use of information technology had lower cost per hospitalization, adjusted for patient severity of illness. It may be that you need a certain economy of scale to implement these systems. Once you have those systems in place your per hospitalization costs are reduced - - overwhelmingly lower. We adjusted for a lot of the characteristics that are typically associated with the higher costs that makes this a robust finding. When you are seeing a patient and have a breadth of options - if you have really sophisticated decision support that is easy to use - - that tool may become an effective agent to help physicians make clinically sound choices that also control costs.
HTN: How much does the effective and extensive use of automation relate to the degree to which physicians are employees of the HCO?
Amarasingham: We didn't look at that particularly. We did look at the hospital organization. We found that the benefits cut across all hospital types. Regardless of the physician practice model, these benefits accrue to the hospital. It’s clearly a challenge for hospitals to ensure that training is provided and protocols followed. If the physicians aren't motivated and engaged with design and training, there’s the potential for very poor outcomes. We didn't look at nursing in our study, but the same applies there as well.
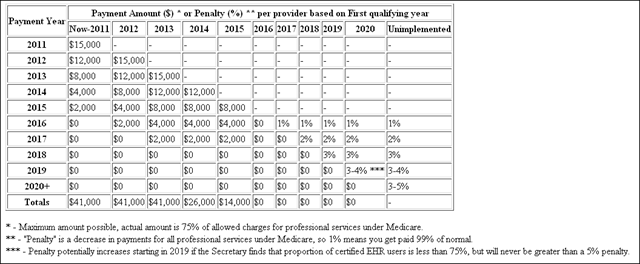
HTN: The stimulus package includes the HITECH Act which includes provisions for federal payments by Medicare and Medicaid for the “meaningful use” of EHRs. As I listen to you talk about CITAT, it strikes me that is exactly what CITAT is measuring.
Amarasingham: Great point. Measuring the presence of technologies would be an inadequate measure. CITAT evaluates whether the 1) technology is present in the organization, 2) the physicians have the know-how to use the technology and 3) the physicians choose to use it over other methods. Government will need to measure some sort of effectiveness outcome like this. Our research suggests that investment in healthcare technology is a wise investment. But it needs to be adopted properly. If it is rushed, not focusing on the socio-technical environment that we discuss in the paper, it could be ineffective. By setting a standard around meaningful use, I think HITECH would be headed in the right direction.










{kind=link}