
It will take a carefully calibrated bi-partisan 60% to get past any Senate filibuster. So what will "careful calibration" look like? Imagine the Steelers' blockers making way for James Harrison's explosive 100 yard interception return. Or imagine the ballet of Santonio Holmes hauling in the winning pass in the far corner of the end zone with 35 seconds to go.

If it passes the Senate, it goes to conference committee to finalize the legislation. We can expect that no changes would be made that risk a Senate challenge to the final bill, like the challenge to a Roethlisberger apparent TD that fell short by 2 inches.
With that in mind, if it passes the Senate we can expect to see many of the following elements in the final bill:
Legislative endorsement for key National Health IT organizations
- Office of National Coordinator for HIT (ONCHIT)
- HIT Policy and Standards Committees through the National eHealth Collaborative (aka AHIC Successor) subject to ONCHIT endorsement.
- Standards and certifications bodies: While unnamed, the Health Information Technology Standards Panel (HITSP) and the Certification Commission for Health Information Technology (CCHIT) are likely beneficiaries in support of standards and certification requirements.
- Electronic exchange and the enterprise integration and use of health information, including establishment and governance of the nationwide health information network (NHIN)
- Utilization of an electronic health record for each person in the United States by 2014.
- Privacy and security protections for the electronic exchange of personally identifiable health information
- Security methods for authorization, authentication and encryption of health information
- Use of health information technology in improving the quality of health care, reducing medical errors, reducing health disparities, improving public health, and improving the continuity of care among health care settings.
- Evaluation of open source health information technology systems for "federal safety net providers".
Financial incentives are tied to "meaningful use" of certified EHR's by physicians and hospitals. "Meaningful use" is defined somewhat circularly in the criteria:
- Use of "EHR technology in a meaningful manner" (which for physician incentives shall include the use of e-prescribing).
- Electronic exchange of health information to improve the quality of care such as promoting coordination of care.
- Reporting on clinical quality measures (which shall become more stringent over time).
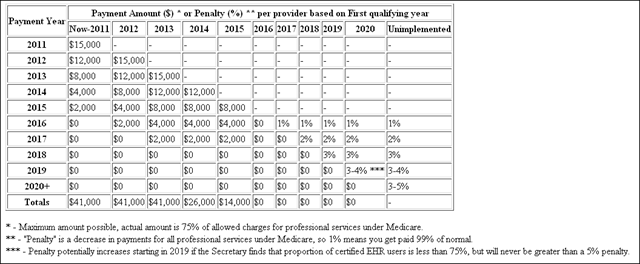
- The Carrot: $41,000 in Medicare payments per eligible physician: Year 1 - $15,000; Year 2 - $12,000; Year 3 - $8,000; Year 4 - $4,000; Year 5 -$2,000. If Year 1 for a professional is 2011 or 2012, then the Year 1 payment is $18,000. No incentive payments if first adopting in 2015. No incentive payments after 2015. Exceptions for rural physicians and later adopters are also specified.
- The Stick: Fee schedule reductions will apply to physicians not using certified EHR technology starting in 2015, with fee schedule reductions of 1% in 2015, 2% in 2016 and 3% in 2017 and beyond.
- These incentives do not apply to hospital-based physicians
- For a summary of this, HISTalk just published a table of bonuses and penalties.
Medicare incentives to hospitals (both carrot and stick) are set up in a similar model as physicians, with a more complex calculation and bigger dollars tied to their meaningful use of certified EHR's. Incentives are calculated based on an initial amount ranging from $2 - 4.6 million (based on number of discharges) multiplied by a Medicare share and a declining "transition factor" for each of four years (1, .75, .5, .25).
Medicaid Incentives
100% federally funded Medicaid incentives are included in the legislation, without back-end reduction in Medicaid fees for non-compliance. Eligible Medicaid physicians are non-hospital based with 30% Medicaid patient volume. Eligible hospitals include 1) children's hospitals, 2) acute care hospitals receiving at least 10% Medicaid patient volume and 3) health centers or rural health clinics with at least 30% Medicaid patient volume.
News Analysis - HITECH's Impact
In a look at the slightly smaller house version of this bill, the Congressional Budget Office (CBO) estimates that $19.8 billion will be spent on HITECH which will, among other things, accelerate adoption of EHR's. The acceleration will deliver US health system net savings of 0.3% betweeen 2011 and 2019, or greater than $60 billion in savings. While this is a good return, 0.3% won't by itself substantially dampen the trajectory of health care spending (see Health Care Costs: A Principal Driver of Long-Term Deficits).
The CBO projects that without the stimulus package "about 45% of hospitals and 65% of physicians will have adopted qualifying health IT in 2019. CBO estimates the incentive mechanism would boost these adoption rates to about 70% for hospitals and about 90% for physicians."
CBO's savings estimates are based on the acceleration of benefits including "reducing the number of inappropriate tests and procedures, reducing paperwork and administrative overhead, and decreasing the number of adverse events resulting from medical errors. Health IT could also improve the quality of care provided to patients by improving the information available to clinicians at the time of treatment, by encouraging the use of evidence based medicine, and by helping physicians manage patients with complex, chronic conditions. The use of health IT could also increase some costs because improved adherence to treatment protocols could increase the amount of care provided."
John Glaser has pointed out that "meaningful use" will need to be clearly spelled out in 2009, leaving only one year for implementation in order for physicians and hospitals to realize the full benefit of the incentive programs. "This is a tall order. And it means that providers should start moving now (if they aren’t already) even though the dust has yet to settle on the specifics."







{kind=link}
No comments:
Post a Comment